SAUNDERS COMPREHENSIVE REVIEW FOR NCLEX ONE
*NURSING > Study Notes > NR566 Week 3 Study Outline (All)
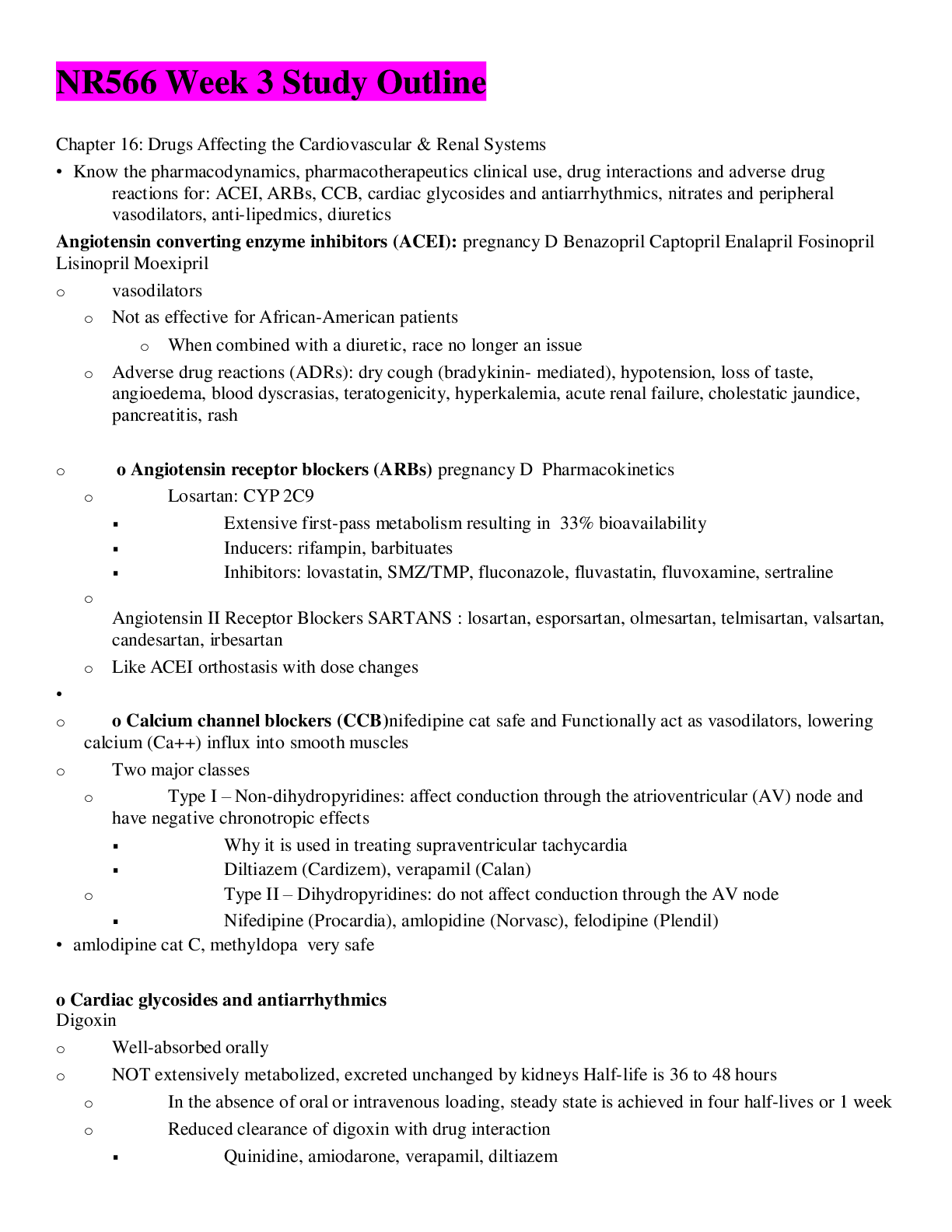
Chapter 16: Drugs Affecting the Cardiovascular & Renal Systems • Know the pharmacodynamics, pharmacotherapeutics clinical use, drug interactions and adverse drug reactions for: ACEI, ARBs, CCB, ... cardiac glycosides and antiarrhythmics, nitrates and peripheral vasodilators, anti-lipedmics, diuretics Angiotensin converting enzyme inhibitors (ACEI): pregnancy D Benazopril Captopril Enalapril Fosinopril Lisinopril Moexipril o vasodilators o Not as effective for African-American patients o When combined with a diuretic, race no longer an issue o Adverse drug reactions (ADRs): dry cough (bradykinin- mediated), hypotension, loss of taste, angioedema, blood dyscrasias, teratogenicity, hyperkalemia, acute renal failure, cholestatic jaundice, pancreatitis, rash o o Angiotensin receptor blockers (ARBs) pregnancy D Pharmacokinetics o Losartan: CYP 2C9 Extensive first-pass metabolism resulting in 33% bioavailability Inducers: rifampin, barbituates Inhibitors: lovastatin, SMZ/TMP, fluconazole, fluvastatin, fluvoxamine, sertraline o Angiotensin II Receptor Blockers SARTANS : losartan, esporsartan, olmesartan, telmisartan, valsartan, candesartan, irbesartan o Like ACEI orthostasis with dose changes • o o Calcium channel blockers (CCB)nifedipine cat safe and Functionally act as vasodilators, lowering calcium (Ca++) influx into smooth muscles o Two major classes o Type I – Non-dihydropyridines: affect conduction through the atrioventricular (AV) node and have negative chronotropic effects Why it is used in treating supraventricular tachycardia Diltiazem (Cardizem), verapamil (Calan) o Type II – Dihydropyridines: do not affect conduction through the AV node Nifedipine (Procardia), amlopidine (Norvasc), felodipine (Plendil) • amlodipine cat C, methyldopa very safe o Cardiac glycosides and antiarrhythmics Digoxin o Well-absorbed orally o NOT extensively metabolized, excreted unchanged by kidneys Half-life is 36 to 48 hours o In the absence of oral or intravenous loading, steady state is achieved in four half-lives or 1 week o Reduced clearance of digoxin with drug interaction Quinidine, amiodarone, verapamil, diltiazem o ADRs o Gastrointestinal (GI) most common: anorexia, nausea/vomiting, diarrhea o Central nervous system: fatigue, disorientation, depression, hallucinations, visual disturbances – yellow vision and green halos around lights o Toxicity: atrial arrhythmias/tachycardia in children o Cardiac: bradycardia, premature ventricular contractions, junctional and AV block arrhythmias, and bigeminy o Avoid using in patients with normal left ventricular systolic function o Monitoring o Diagnosis of toxicity is based on both clinical and laboratory data o Toxicity commonly occurs with serum levels greater than 2 ng/mL o Monitor potassium levels • • o Nitrates and peripheral vasodilators nitrates work on veins and reduce preload, hydralazine is a vasodilator • o Anti-lipidemics • o Diuretics treat symptoms of congestions, help the body get rid of excess fluid, reduce symptoms that result in excess fluids like shortness of breath doing this it reduces heart failure (aldosterone inhibitors) • Also know: • o ACEIs & ARBs benefits in other conditionsHTN, HEART FAILURE, SLOWING RENAL DISEASE , CARDIOVASCULAR DISEASE AS WELL • o Dosing schedules • o Management of ACEI side effects • o Therapeutic monitoring for cardiac glycosides and antiarrhythmics • Chapter 28: Chronic Stable Angina & Low Risk Unstable Angina Differentiate between myocardial oxygen supply & demand Angina: Ischemia caused by the imbalance between myocardial oxygen supply (MOS) and myocardial oxygen demand (MOD) produces pain referred to as angina. • Ischemia occurs when demand exceeds supply • Chronic stable angina (exertional angina) is caused by narrowing of the arterial lumen and hardening of the arterial walls so that the affected vessels cannot dilate in response to the increased MOD associated with physical exertion or emotional stres Etiology, diagnosis and risk factors The major risk factors for CAD are age, family history, smoking, hypertension, hypercholesterolemia, low HDL cholesterol, and diabetes mellitus. These risk factors are used in the Framingham equations for calculating the 10-year risk for the development of coronary heart disease (Anderson et al, 2007) and in the new risk equations that aim at uncovering a 7 year risk In addition, conditions that decrease oxygen supply and increase oxygen demand are also major risk factors for ischemic heart disease. These include heart failure anemia), hypertension (hyperthyroidism), valvular heart disease, and morbid obesity. • There are also noncardiac disorders that mimic angina because their primary symptom is chest pain. These include pulmonary embolism, pneumonia, pneumothorax, gastroesophageal spasm or reflux, cholecystitis, peptic ulcer, pancreatitis, rib fractures, herpes zoster, and panic disorder. Some of these disorders also decrease oxygen supply and can cause angina • Women often have symptoms of angina that are atypical and may include fatigue, shortness of breath without chest pain, nausea and vomiting, back pain, jaw pain, dizziness, and weakness ( Grading criteria for levels of angina The lower the class, the more likely the patient's angina can be controlled by lifestyle modification and intermittent nitroglycerin (Table 28-2). The higher the class, the more likely the patient will require multiple drug therapy. The ACC/AHA guidelines have a classification system that incorporates the NYHA/CCS syst [Show More]
Last updated: 3 years ago
Preview 1 out of 17 pages
Buy this document to get the full access instantly
Instant Download Access after purchase
Buy NowInstant download
We Accept:

Can't find what you want? Try our AI powered Search
Connected school, study & course
About the document
Uploaded On
Sep 10, 2021
Number of pages
17
Written in
All
This document has been written for:
Uploaded
Sep 10, 2021
Downloads
0
Views
102
Scholarfriends.com Online Platform by Browsegrades Inc. 651N South Broad St, Middletown DE. United States.
We're available through e-mail, Twitter, and live chat.
FAQ
Questions? Leave a message!
Copyright © Scholarfriends · High quality services·