Mark Klimek Lectures 1 to 12 for High Scoring Grades
Document Content and Description Below
Lecture 1— Acid-Base Balance
Ventilators
Lecture 2— Alcohol
Wernicke
Overdose and Withdrawal
S/Sx
Aminoglycosides
Peak and Trough
Lecture 3— Drug Toxicities (Lithium,
Lanoxin, Dilantin, Bilirubin,
Aminophylline
...
[Show More]
Last updated: 4 months ago
Preview 1 out of 92 pages
Instant download

Buy this Document to get the Full Access Instantly
Provided by Students Who Aced it
We Verify Document Content to Gurantee Accuracy
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Aug 14, 2021
Number of pages
92
Written in
All

Additional information
This document has been written for:
Uploaded
Aug 14, 2021
Downloads
0
Views
135
Document Keyword Tags
Recommended For You
Get more on NCLEX »
$9
92 Pages
Mark Klimek Lectures 1 to 12: The Guide.Latest (Best,Graded A)
$16
92 Pages
Mark Klimek Lectures 1 to 12 Complete Study Guide. A+ Guide.
$10
92 Pages
Mark Klimek Lectures 1 to 12 Complete Study Guide a guide 2023
$10
92 Pages
Mark Klimek Lectures 1 to 12 Complete Study Guide a guide 2023
$16
92 Pages
Mark Klimek Lectures 1 to 12 Complete Study Guide a guide 2023
$15
92 Pages
Mark Klimek Lectures 1 to 12 Complete Study Guide a guide 2023
$11
92 Pages
Mark Klimek Lectures 1 to 12: The Guide.Latest (Best,Graded A)
$14
92 Pages
Mark Klimek Lectures 1 to 12: The Guide. Complete Study Guide...

$15
93 Pages
Mark Klimek Lectures 1 to 12: The Guide.Latest (Best,Graded A)
$12
866 Pages
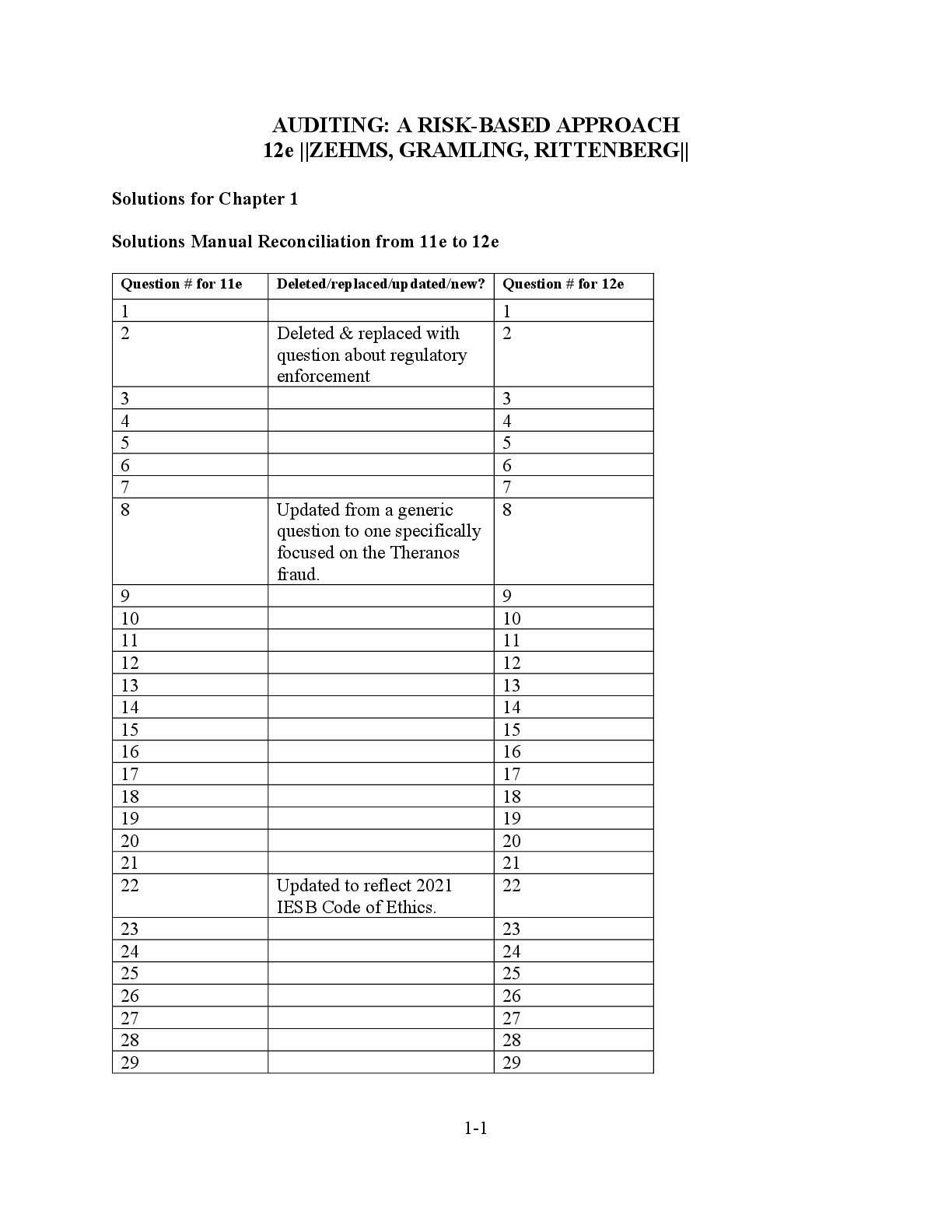
AUDITING: A RISK-BASED APPROACH 12e ||ZEHMS, GRAMLING, RITTENB...

$11
92 Pages
Exam (elaborations) Mark Klimek Lectures 1 to 12: The Guide.La...
$23
111 Pages
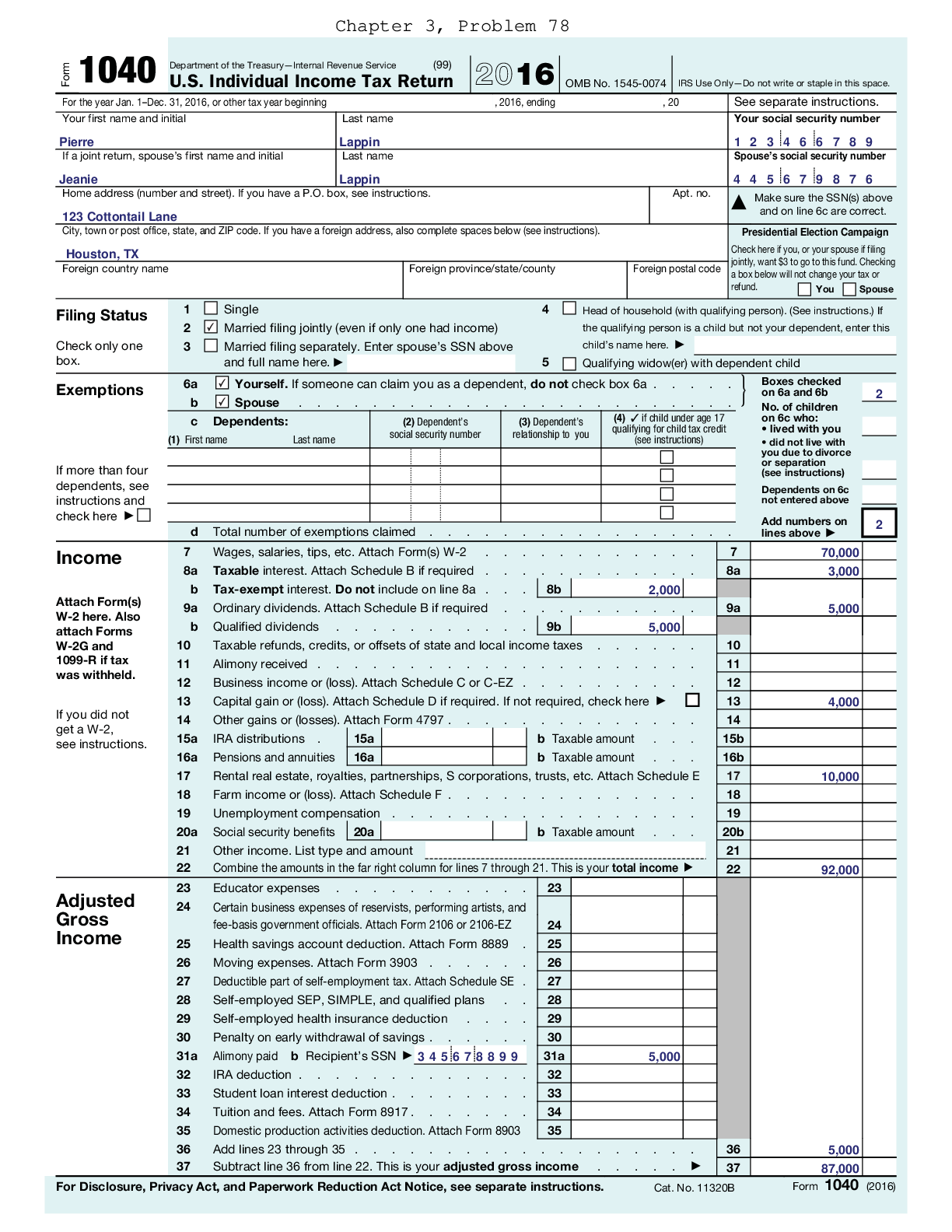
DEVELOP RESEARCH SKILLS PROBLEMS TAXATION FOR DECISION MAKERS...
$20.5
841 Pages
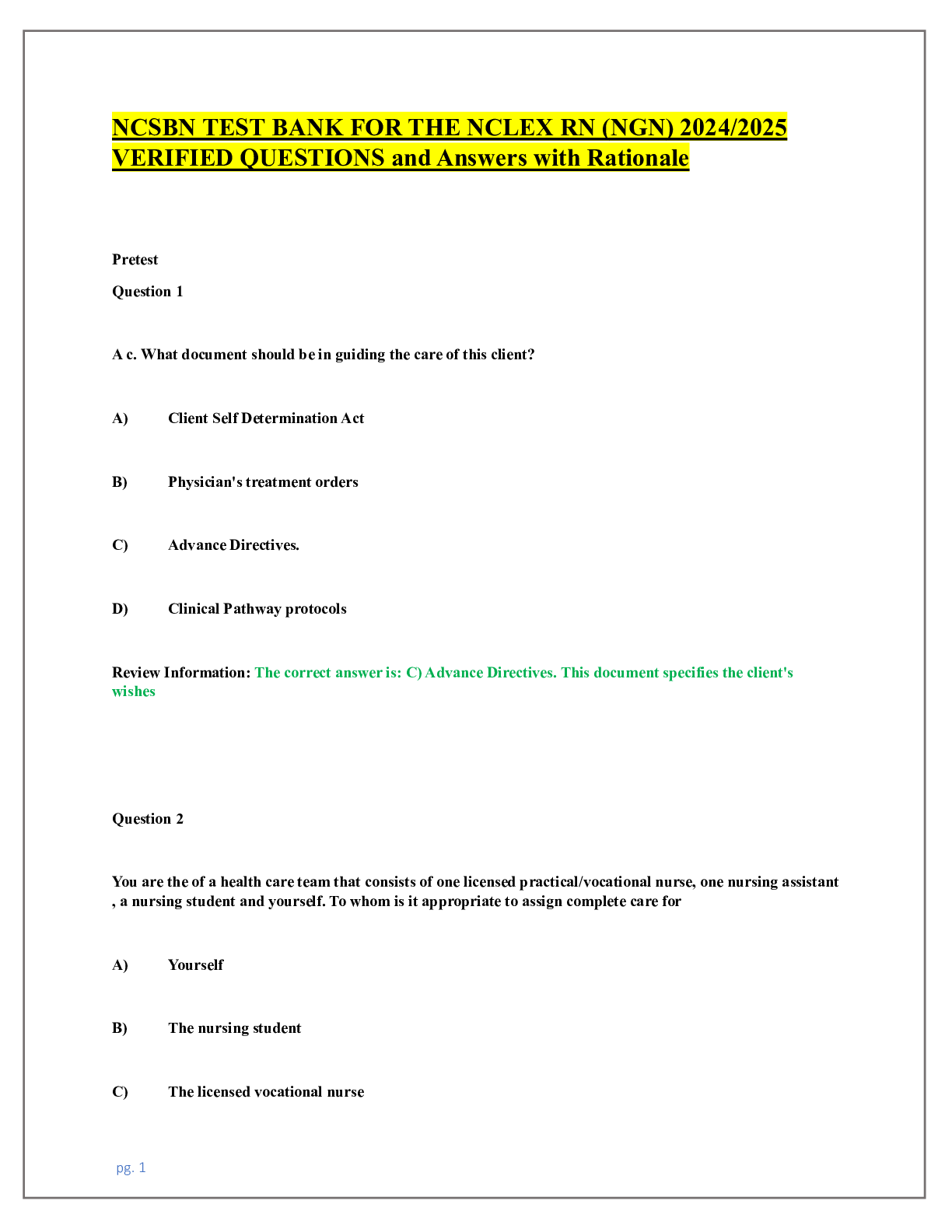
NCSBN TEST BANK FOR THE NCLEX RN (NGN) 2024/2025 VERIFIED QUES...

$22
1219 Pages
NCSBN TEST BANK for the NCLEX-RN & NCLEX-PN UPDATED Question...
More related documents below

.png)
.png)




 Kathryn Cadenced Colgrove, Christi Doherty - Pharmacology Success_ NCLEX®-Style Q&A Review-F.png)
 (1).png)
