Diagnosis – Ectopic pregnancy
DDX – Endometriosis, tubo-ovarian abcess, Pelvic inflammatory disease, ovarian cyst, ectopic pregnancy, abortion, ovarian torsion, dysmenorrhea-primary
Problem Statement:
( Demographic de
...
Diagnosis – Ectopic pregnancy
DDX – Endometriosis, tubo-ovarian abcess, Pelvic inflammatory disease, ovarian cyst, ectopic pregnancy, abortion, ovarian torsion, dysmenorrhea-primary
Problem Statement:
( Demographic description – chief complaint – Hx and PE key findings – risk factors )
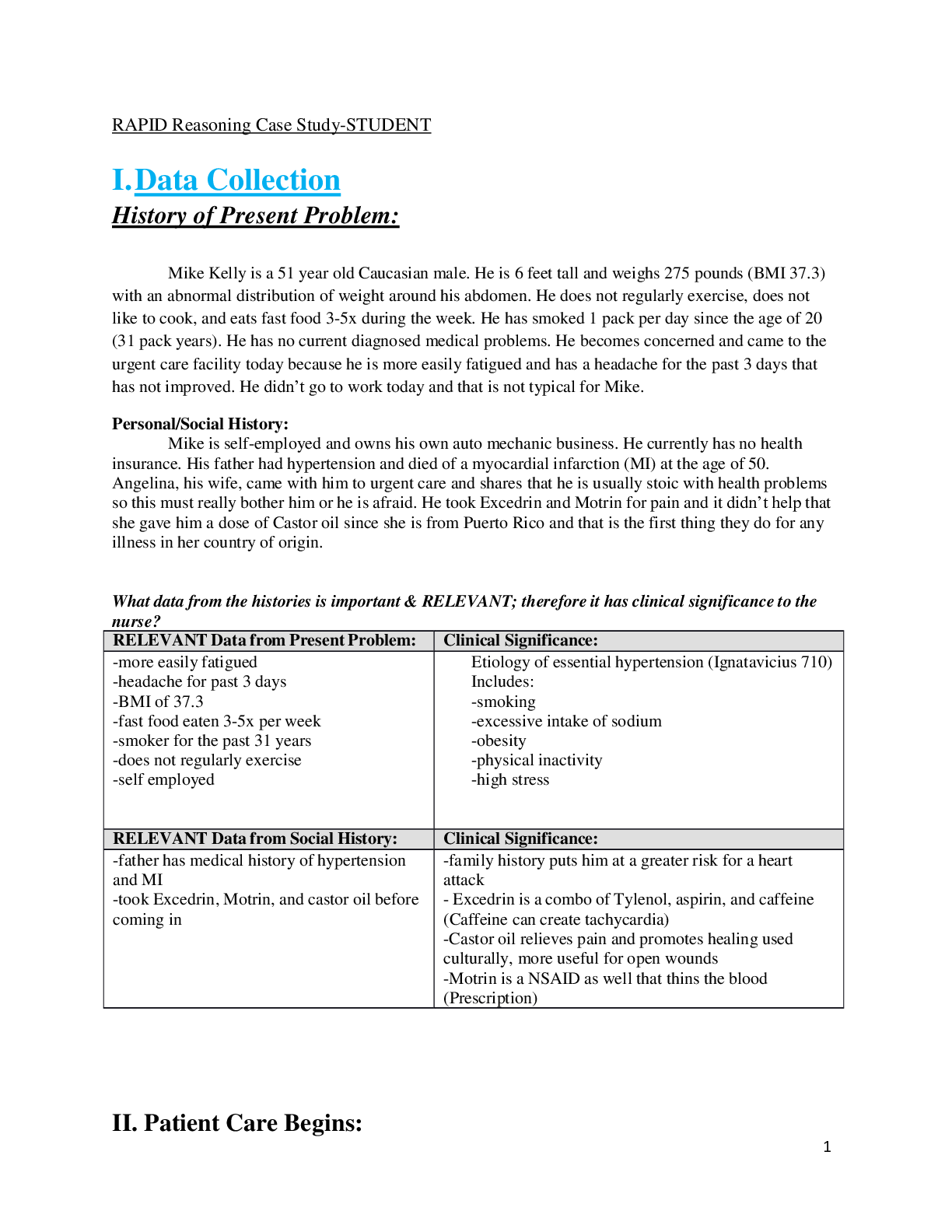
Pamela Flowers is a 24 year old G0P0 woman presenting with abnormal vaginal bleeding and LLQ pelvic pain for 1 day. She has a history of dysparenuria on her left side. Gynecological exam shows tenderness and L- adnexal fullness (no mass) w/ enlarged + soft uterus. Patient has history of irregular periods.
( you just need a treatment plan )
CC: Pamela Flowers is a 24 year old G0P0 woman presenting with abnormal vaginal bleeding and LLQ pelvic pain
HPI: The vaginal bleeding and pain started 1 day prior. Patient also describes dyspareunia 1 week ago, and has history of ‘irregular periods’
Meds: inhaler for asthma
PMH: Pap smear + gyn exam 8mo ago normal – treated for chlamydia infection 3 years ago.
SH: one current sexual partner, condoms for contraception.
ROS: Only positive findings are seen in HPI
Physical Exam:
VS: Pulse – 104; BP – 108/60 RR – 14; T – 98.8F (37 C); SpO2 – 98%
Gynecologic: Tenderness noted to bimanual exam. Left Adnexal fullness seen without mass. Uterus is enlarged and softened.
ASSESSMENT/PLAN
Test Results:
• Human chorionic gonadotropin (hCG), plasma: Value consistent with 5-6 w normal gestation, suggest transvaginal ultrasound.
• TVUS: high probability of left fallopian tube ectopic pregnancy
• LFTs: Normal (allows her to be Methotrexate candidate)
Management Plan
• Methotrexate
• Monitor b-hCG levels after 1 week of MTX.
• If no improvement consider salpingostomy / salpingectomy
...............................................CONTINUED.........................................
[Show More]