Focused Exam: Abdominal Pain Results | Turned In
Advanced Health Assessment - Chamberlain, NR509-April-2018
Return to Assignment
Your Results Lab Pass
Documentation / Electronic Health Record
Document: Vitals Docume
...
Focused Exam: Abdominal Pain Results | Turned In
Advanced Health Assessment - Chamberlain, NR509-April-2018
Return to Assignment
Your Results Lab Pass
Documentation / Electronic Health Record
Document: Vitals Document: Provider Notes
Document: Provider Notes
Student Documentation Model Documentation
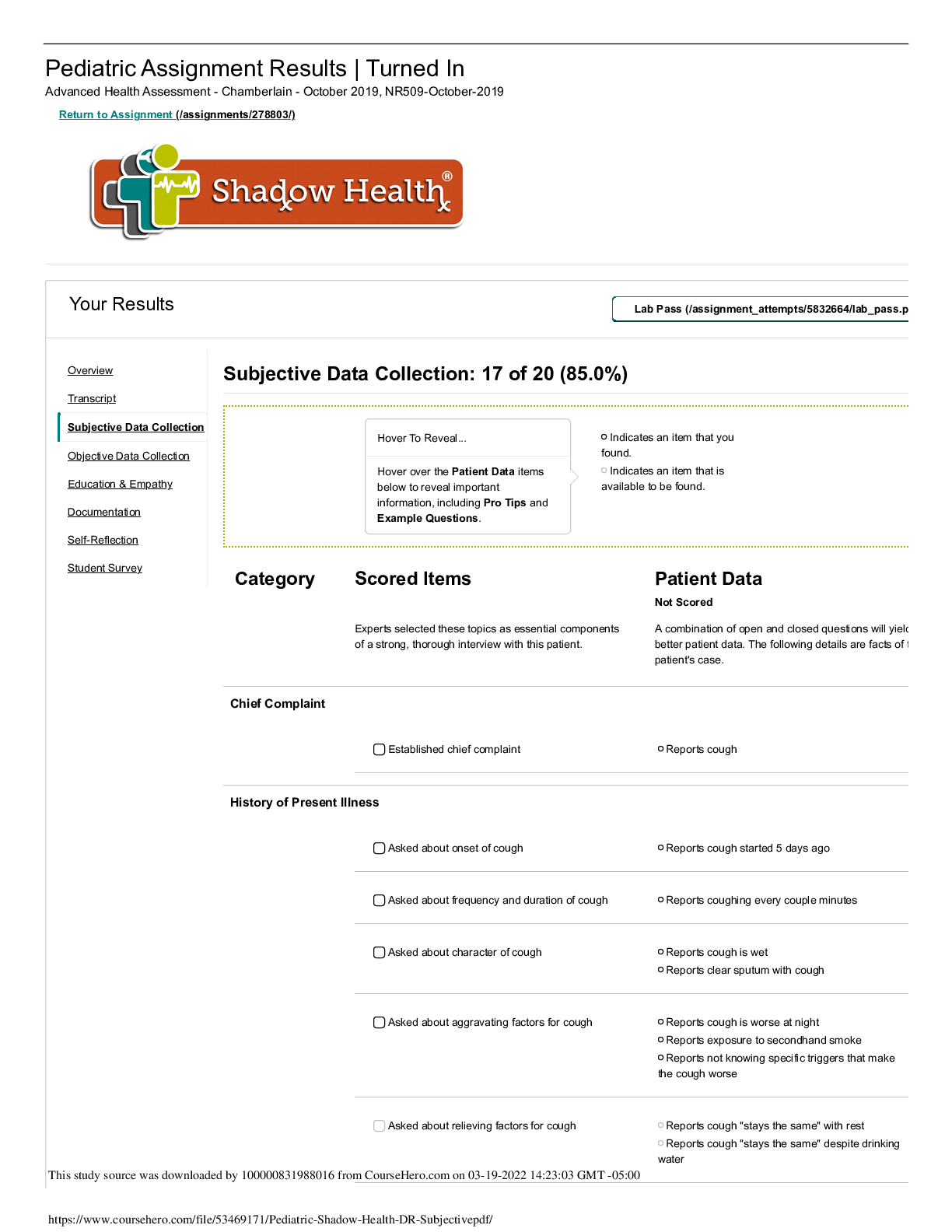
Subjective
Miss Park is a 78 year old female of Korean to send
date of birth Jan 17.
CC Miss Park States" I have some pain in my belly
and I am having difficulty going to the bathroom my
daughter was worried about me."
C: pain in belly with difficulties going to the
bathroom, dull crampy feeling. 6/10 on pain sacele
O: 5 days ago, gradual, constant and bloating
L: lower belly, entire bellly
D: constant pain
E: moivng and eating , has missed both of her
exercise classes and states " never misses her
exercise classes."
R: resting helps a little but no real relief, sips of
warm water a friend suggested not helping
R: patient has not tried any medication, aggravated
with eating and physical activity also reports low
energy level, a dull crampy feeling a 6 out of 10 on
the Pain Scale.
A: Bowel movement noted a few days ago was
diarrhea, denies any history of constipation. Reports
having diarrhea about 2 to 3 days ago sudden onset
lasting one day, record very loose and watery:
normal normal bowel movements description of
brown formed and soft are usually every day until 5
days ago. Reports recent slight decrease in
frequency of urination do to decrease water intake.
Urine darker than usual. Denies blood in urine.
Denies any GI history disorders. Denies history of
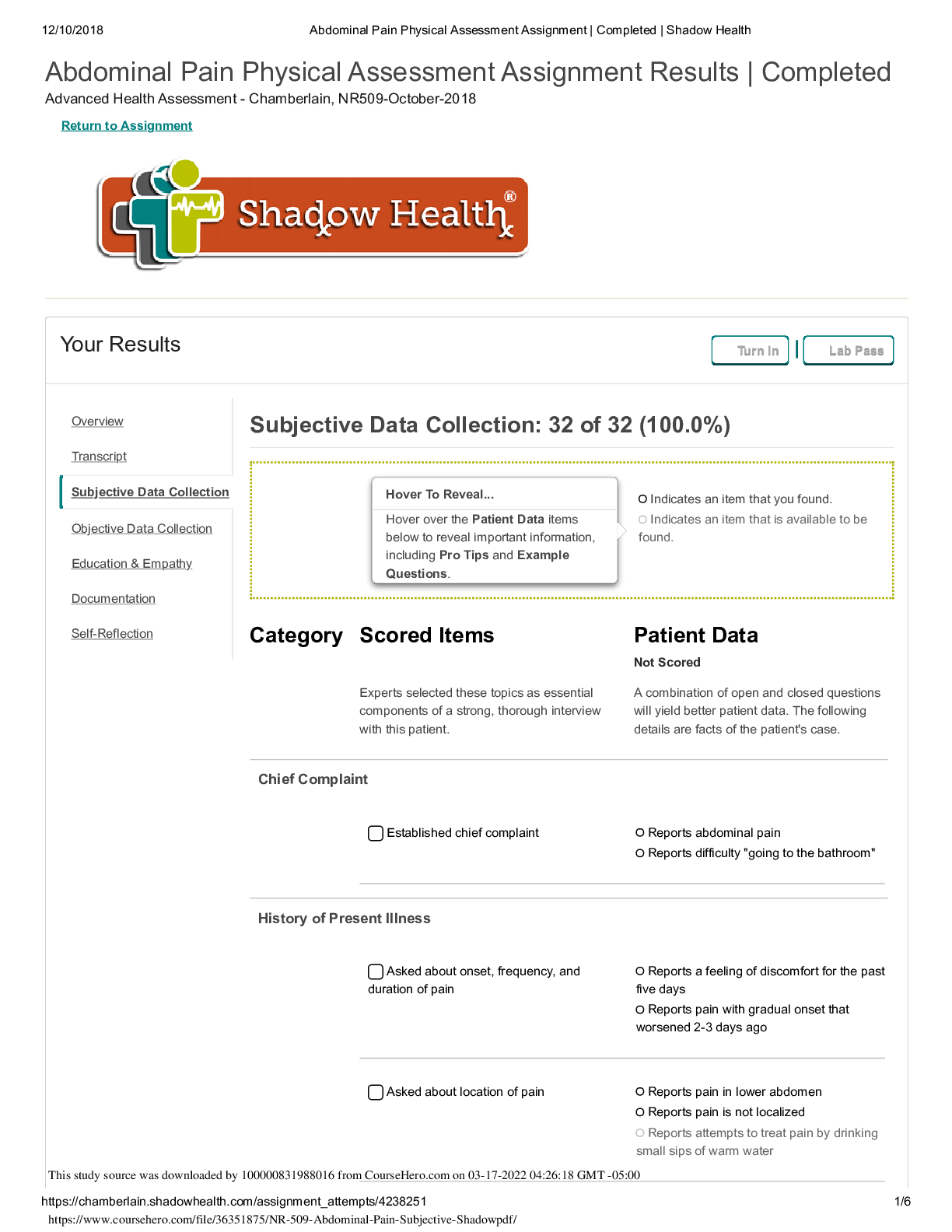
Ms. Park reports that she is “having pain in her
belly.” She experienced mild diarrhea three days
ago and has not had a bowel movement since. She
reports that she has been feeling some abdominal
discomfort for close to a week, but the pain has
increased in the past 2-3 days. She now rates her
pain at 6 out of 10, and describes it as dull and
crampy. She reports her pain level at the onset at 3
out of 10. She is also experiencing bloating. She did
not feel her symptoms warranted a trip to the clinic
but her daughter insisted she come. She describes
her symptoms primarily as generalized discomfort in
the abdomen, and states that her lower abdomen is
the location of the pain. She denies nausea and
vomiting, blood or mucus in stool, rectal pain or
bleeding, or recent fever. She denies vaginal
bleeding or discharge. Reports no history of
inflammatory bowel disease or GERD. Denies family
history of GI disorders. Her appetite has decreased
over the last few days and she is taking small
amounts of water and fluids. Previously she reports
regular brown soft stools every day to every other
day.
Overview
Transcript
Subjective Data Collection
Objective Data Collection
Education & Empathy
Documentation
Self-Reflection
5/28/2018 Focused Exam: Abdominal Pain | Completed | Shadow Health
GERD heartburn or ulcers. No history of
appendicitis, stomach cancer, or history of liver
disease. Report C-section at age 40 in
cholecystectomy at age 42 no post-op
complications noted. Last pap smear noted about
10 years ago
Current medications: Accupril 10 po QD( last dose
at (0800 this morning), denies any OTC medications
Allergies: Latex : contact dermatitis
PMHx:
1. Hypertension diagnosed at age 54
2.3 Pregnancies
4. Surgical history C-section at age of 40;
cholecystectomy at age 42
Reports hospitalizations for past surgeries as noted
above and after childbirth denies any other
hospitalizations. Last pap smear and colonoscopy
10 years ago.
SocHx:
Last meal with toast for breakfast not eating well.
Usually appetite is three meals a day does not eat
snacks. Typical meal for breakfast is usually some
sort of fruit usually a banana. Typical lunch is usually
soup reports sometimes skipping lunch period and
typical dinner is chicken or fish with some sort of
rice or vegetable. No fiber supplements reported.
Patient reports believes gets enough fiber supports
eating a vegetable or fruit each day. Reports
decrease in thirst especially over the last few days
typically patient drinks 6 typically patient drink 6
denies caffeinated drinks such as coffee or soda on
occasion drinks chamomile tea. Deny sexual activity
reports no STI testing. Report moderate activity
attend Fitness classes and reports gardening as a
hobby. Lives with her daughter named Jennifer and
has a strong support system with her daughter and
gentleman friend Max denies any recent travel.
Report sexually active no vaginal intercourse
reported does report oral sex.
1. No past or present tobacco use
2. Reports drinking one alcoholic (wine)beverage
per week, 4 per month only on Sunday's white wine
3. Denies using marijuana, cocaine, heroin or illicit
drugs
FAM Hx:
1. Mother- deceased at age 88 history of
hypertension and Diabetes Type 2
2. Father: deceased at 82 history of hypertension
and hypercholesterolemia
3. Maternal grandparents: family history of coronary
artery disease and Diabetes Type 2
4. Paternal grandparents: history of obesity, CVA,
hypertension
5. Siblings: brother had history of hypertension,
hypercholesterolemia, prostate cancer
6. Son: healthy age 48
7. Daughter: healthy age 46
ROS:
General: denies any recent fever chills or night
sweats although patient does report short-term
feeling of tiredness I need to rest more often.
GI: reports bloating, slight increase in flatus, recent
loss of appetite. No reports of nausea vomiting or
5/28/2018 Focused Exam: Abdominal Pain | Completed | Shadow Health
recent weight changes or possible food exposure
for food poisoning.
GU: denies painful urination no burning upon
urination no urinary incontinence no history of UTIs
no gynecological problems no vaginal bleeding no
vaginal discharge onset of menopause 54. Reports
no history of kidney or bladder problems.
Respiratory: patient denies any sore throat, cough,
dysphagia, difficulty breathing, chest pain or chest
tightness. Denies any change of taste.
Objective
VS
B/P: 110/70 mmhg ( MAP 83 mmhg)
HR: 92
RR: 16
Temp: 37.2 C ( 98.6 F)
Pain 6/10 on pain scale
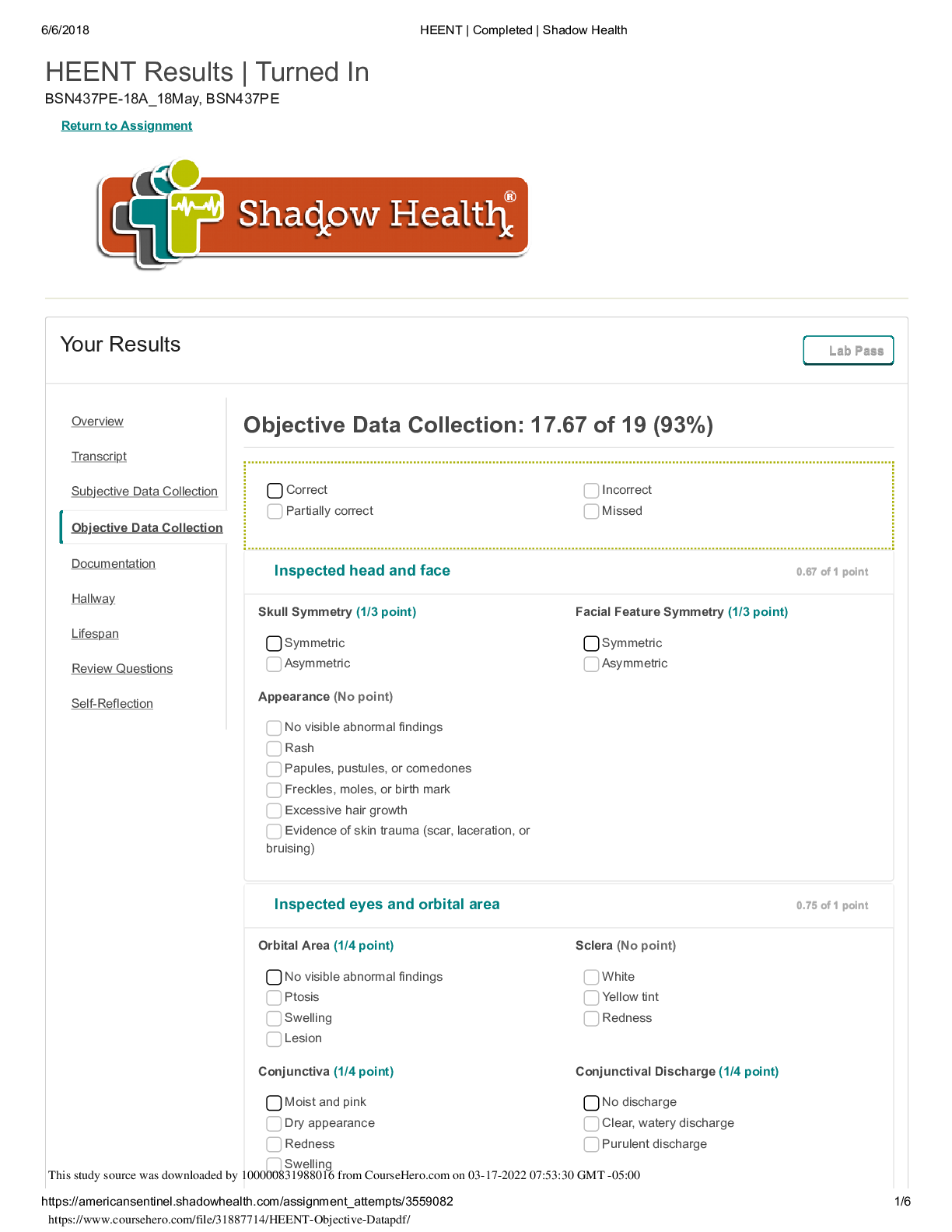
Inspection:
Inspection Head and face- flight flushing of the
cheeks
Inspection Nose- dry appearance
Inspection Mouth and throat- dry appearance
Inspection Abdominal- scarring noted
approximately 6 in a scar to the right upper
quadrant and a approximately 10-cm scar at midline
Supra pubic region
Inspection Lower extremities- inspected lower
extremities for edema no edema noted bilaterally.
Ausculte
Auscultate Heart sounds- S1 and S2 audible no
extra sounds
Auscultate Breath sounds- present in all areas no
adventitious sounds all clear
Auscultate Abdominal aorta- no bruit
Auscultate bowel sounds- Normoactive active all
quadrants
Auscultate Abdominal arteries- no Brit noted
bilateral renal, iliac or femoral
Auscultated organs- over spleen and liver no friction
rubs noted
Percussion
Percuss abdomen: dullness noted to the left lower
quadrant and tympany and all other quadrants
percuss spleen: Tympany noted
Percuss liver span: approximately 7 cm in the
midclavicular line
Pecuss CVA tenderness: no reaction noted bilateral
flank
Palpation:
Light abdominal palpation:
Right lower quadrant with light pressure no
tenderness noted no guarding or distention no
masses. Palpated left lower quadrant with light
pressure tenderness reported palpable guarding
and distention no masses. Palpated left upper
quadrant with light pressure noted as reported no
masses, Guarding, or distention. Palpated right
upper quadrant with light pressure no tenderness
reported, no masses, Guarding, or distention
Deep abdominal palpation: palpated upper right
quadrant with deep pressure no masses. Palpated
• General Survey: Uncomfortable and flushed
appearing elderly woman seated on exam table
grimacing at times. Appears stable but mildly
distressed.
• HEENT: Mucus membranes are moist. Normal skin
turgor; no tenting.
• Cardiovascular: S1, S2, no murmurs, gallops or
rubs; no S3, S4 rubs. No lower extremity edema.
• Respiratory: Respirations quiet and unlabored,
able to speak in full sentences. Breath sounds clear
to auscultation.
• Abdominal: 6 cm scar in RUQ and 10 cm scar at
midline in suprapubic region. An abdominal exam
reveals no discoloration; normoactive bowel sounds
in all quadrants; no bruits; no friction sounds over
spleen or liver; tympany presides with scattered
dullness over LLQ; abdomen soft in all quadrants;
an oblong mass is noted in the LLQ with mild
guarding, distension; no organomegaly; no CVA
tenderness; liver span 7 cm @ MCL; no hernias.
[Show More]
.png)









.png)