NR-507 Mid-Term Study Guide
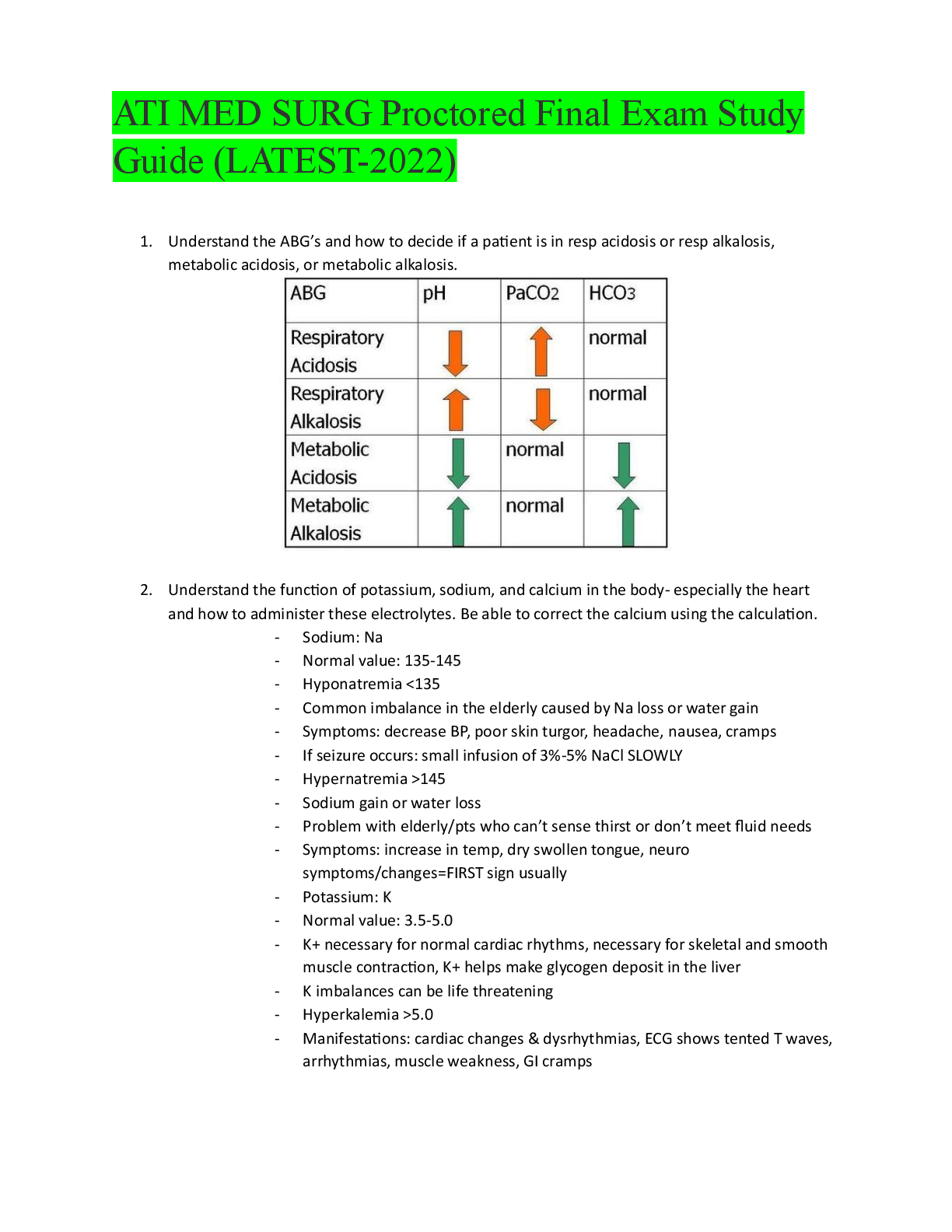
Hello Class,
This study guide is for the 50 question multiple choice Mid-Term exam that will be given
during Week 4. It will cover the following concepts:
Pulmonary: review concepts relate
...
NR-507 Mid-Term Study Guide
Hello Class,
This study guide is for the 50 question multiple choice Mid-Term exam that will be given
during Week 4. It will cover the following concepts:
Pulmonary: review concepts related to anticholinergic drugs and the treatment
for asthma,
bronchitis and associated pathogenesis; We are now ready to address the
pathogenesis of chronic bronchitis which begins with some sort of exposure to airborne
irritants which activates bronchial smooth muscle constriction,
mucus secretion, and release of inflammatory mediators (histamine, prostaglandins,
leukotrienes, interleukins) from immune cells located in the lamina propria
These airborne irritants can include air pollution or industrial chemicals & fumes. But
the most common irritant is smoke from cigarettes and other tobacco products.
Keep in mind that all of these bronchial responses are, in fact, normal responses
to occasional inhalation of airborne irritants.
Smooth muscle constriction is important to limit passage of the irritant deeper into the
respiratory tract.
Secretion of mucus and release of inflammatory chemicals are also important to help
trap and defend against a potential harmful substance.
The transition from a normal, protective respiratory response to a detrimental effect
occurs with ….
long-term exposure to airborne irritants which promotes
smooth muscle hypertrophy à increased bronchoconstriction
hypertrophy and hyperplasia of goblet cells à mucus hypersecretion
epithelial cell metaplasia à non-ciliated squamous cells
migration of more WBCs to site à inflammation & fibrosis in bronchial wall
thickening and rigidity of bronchial basement membrane à narrowing of bronchial
passageways
chronic bronchitis and related acid/base disturbances, Because of the anatomical
changes in the bronchioles associated with chronic irritation ventilation, especially
exhalation, is compromised.
Pressure differences during inhalation are high enough to force air into the alveoli.
However, during exhalation the narrowing and collapse of the air passageways causes
air to be trapped in the alveoli resulting in.
alveolar hyperinflation à expanded thorax
hypercapnia (CO2 retention) à respiratory acidosis
What is chronic bronchitis?
This is a chronic disease characterized by:
bronchial inflammation,
hypersecretion of mucus, and
chronic productive cough, persisting for at least 3 consecutive months for
at least 2 successive years
Chronic bronchitis is caused by:
long-term exposure to environmental irritants,
repeated episodes of acute bronchitis (infection), and
factor(s) affecting gestational or childhood lung development – the most
common being pre-term birth and/or RSV infection in early infancy
Chronic bronchitis results in:
excess mucus production and accumulation,
hypertrophy of bronchial smooth muscle,
hypertrophy & hyperplasia of bronchial mucus-producing cells,
airflow obstruction, and
decreased alveolar ventilation
The lung damage from chronic bronchitis is typically considered irreversible.
The most common symptoms of chronic bronchitis are:
productive, purulent cough
copious sputum production
shortness of breath
wheezing, rhonchi – sounds typically associated with fluid/mucus in the airways
cyanosis – bluish discoloration of the skin and mucous membranes associated
with poor oxygenation
peripheral edema
perfusion, he high concentration of CO2 creates unfavorable conditions for gas
exchange, so there is
decreased O2 exchange à ventilation/perfusion (V/Q) mismatch
Decreased perfusion of the pulmonary capillaries with oxygenated blood results in
chronic pulmonary hypoxia à cyanosis
(the term “blue bloater” used to describe a client with chronic bronchitis, with bloater
referring to the expanded thorax that these individuals can develop as a result of
alveolar hyperinflation)
Poor ventilation, leading to decreased perfusion, causes Right to Left “shunting” to
occur. This is the phenomenon where deoxygenated blood passes from the RV to lungs
to the LV without adequate perfusion (gas exchange)
Perfusion, the actual exchange of O2 and CO2 in the bloodstream, occurs via the alveoli
and pulmonary capillaries.
Ventilation, air movement in/out of the lung, is critical to ensure sufficient perfusion.
blood flow between the heart and lungs,
Blood enters the heart through two large veins, the inferior and superior vena cava,
emptying oxygen-poor blood from the body into the right atrium. ... As the ventricle
contracts, blood leaves theheart through the pulmonic valve, into
the pulmonary artery and to the lungs where it is oxygenated.Feb 4, 2019
asthma signs and symptoms,
The most common symptoms of both extrinsic and intrinsic asthma are: coughing,
wheezing shortness of breath rapid breathing chest tightness, difficulty breathing/
bronchioles, After air enters the nasal and/or oropharynx it passes into the trachea
which branches into Left & Right bronchi, which further divide into smaller passageways
called the bronchioles, and finally almost 30 branch points later, form the actual gas
exchange areas called the alveoli
The bronchioles or bronchioli are the smaller branches of the bronchial passageways in
the respiratory tract that deliver air to the smaller terminal bronchioles in the conducting zone, and
even smaller respiratory bronchioles in the respiratory zone. The bronchioles no longer contain the
cartilage, that is found in the bronchi, or glands in their submucosa
[Show More]











.png)
.png)