NURSING > STUDY GUIDE > NR511 Final Exam Study Guide (All)
NR511 Final Exam Study Guide
Document Content and Description Below
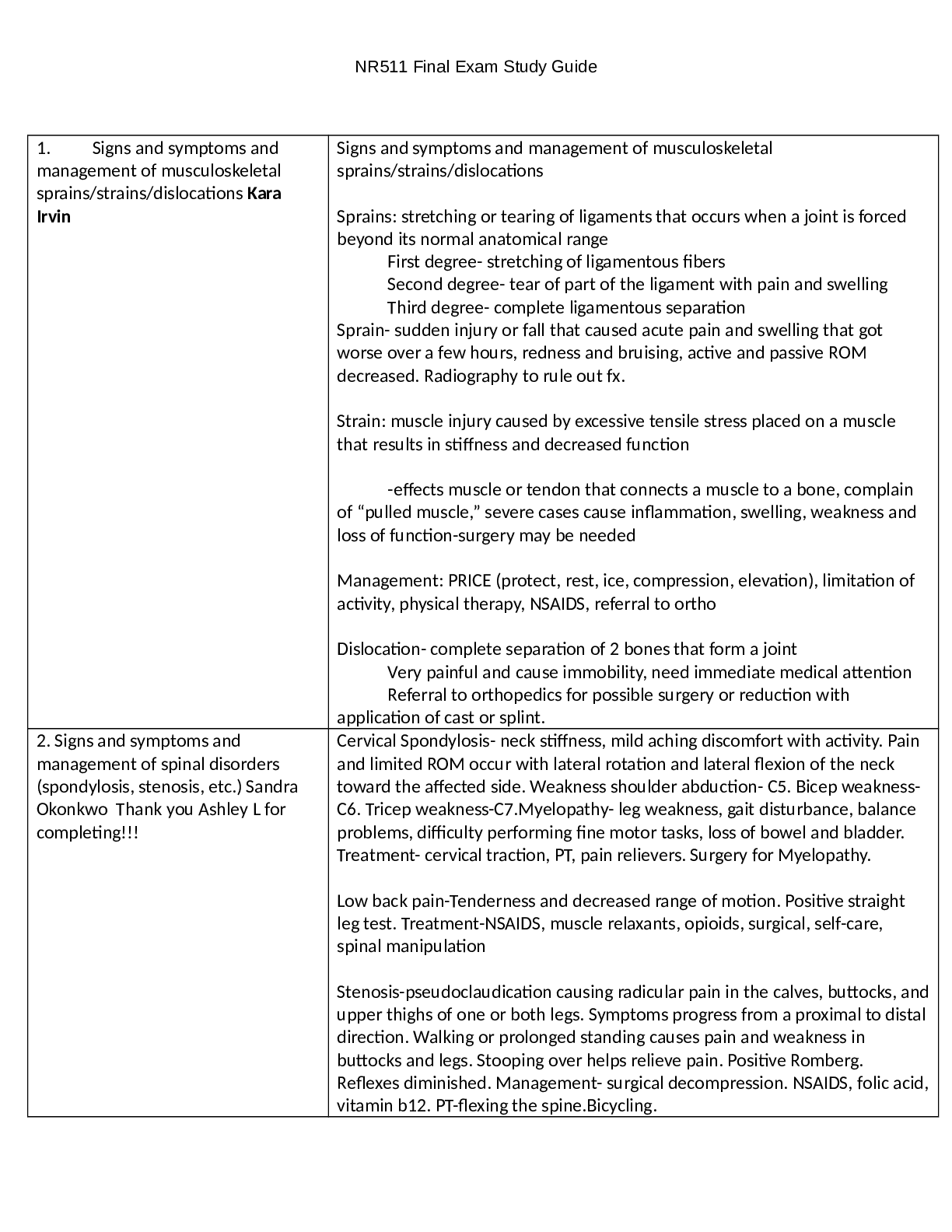
NR511 Final Exam
Study Guide
See Midterm and Week 1 Study Guide for content covering weeks 1, 2 & 3
Common Infections
1. Impetigo
Impetigo is a superficial bacterial infection of the skin. It is classified into prim
...
[Show More]
Last updated: 3 years ago
Preview 1 out of 74 pages
Instant download

Buy this document to get the full access instantly
Instant Download Access after purchase
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jun 19, 2022
Number of pages
74
Written in
All

Additional information
This document has been written for:
Uploaded
Jun 19, 2022
Downloads
0
Views
258
Document Keyword Tags
Recommended For You
Get more on STUDY GUIDE »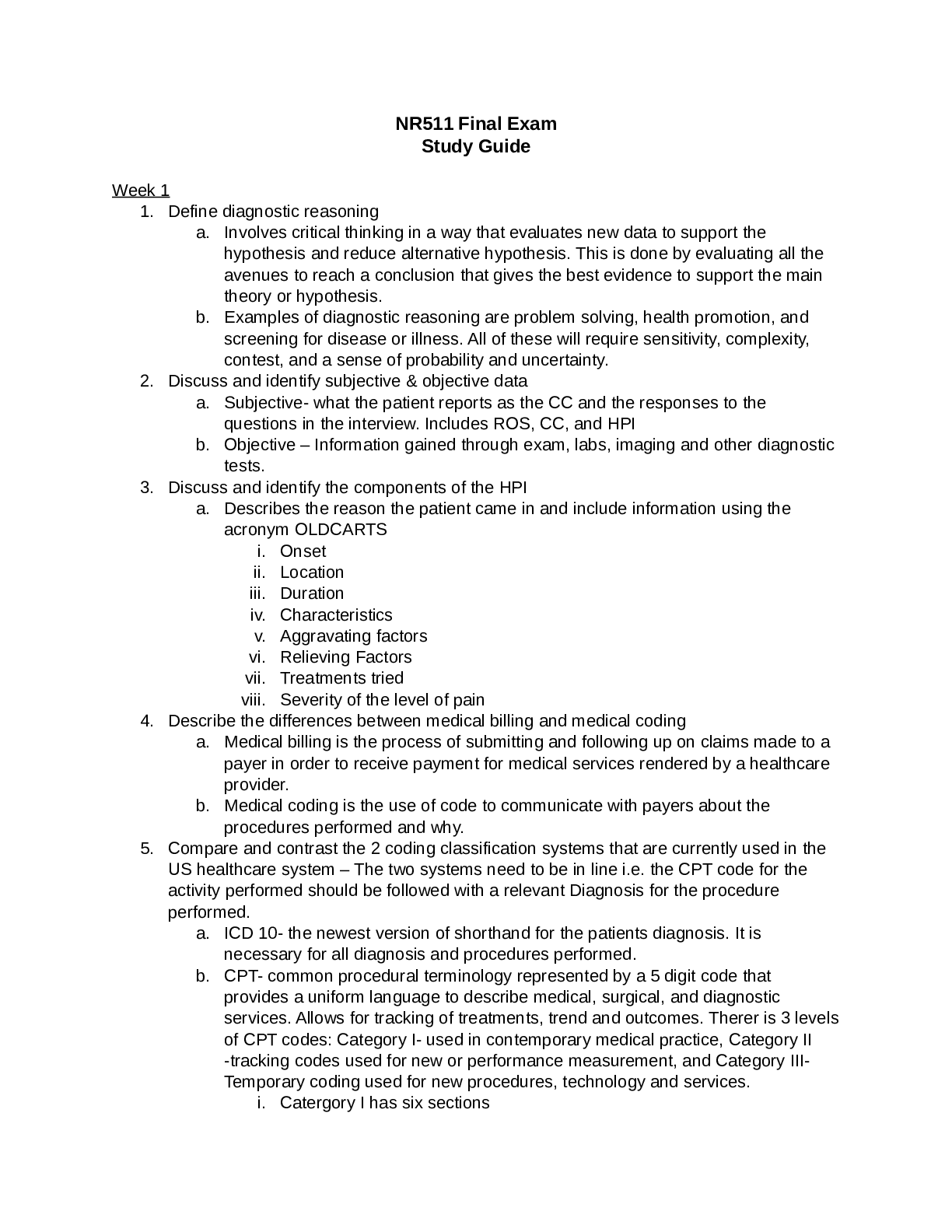

$18
234 Pages
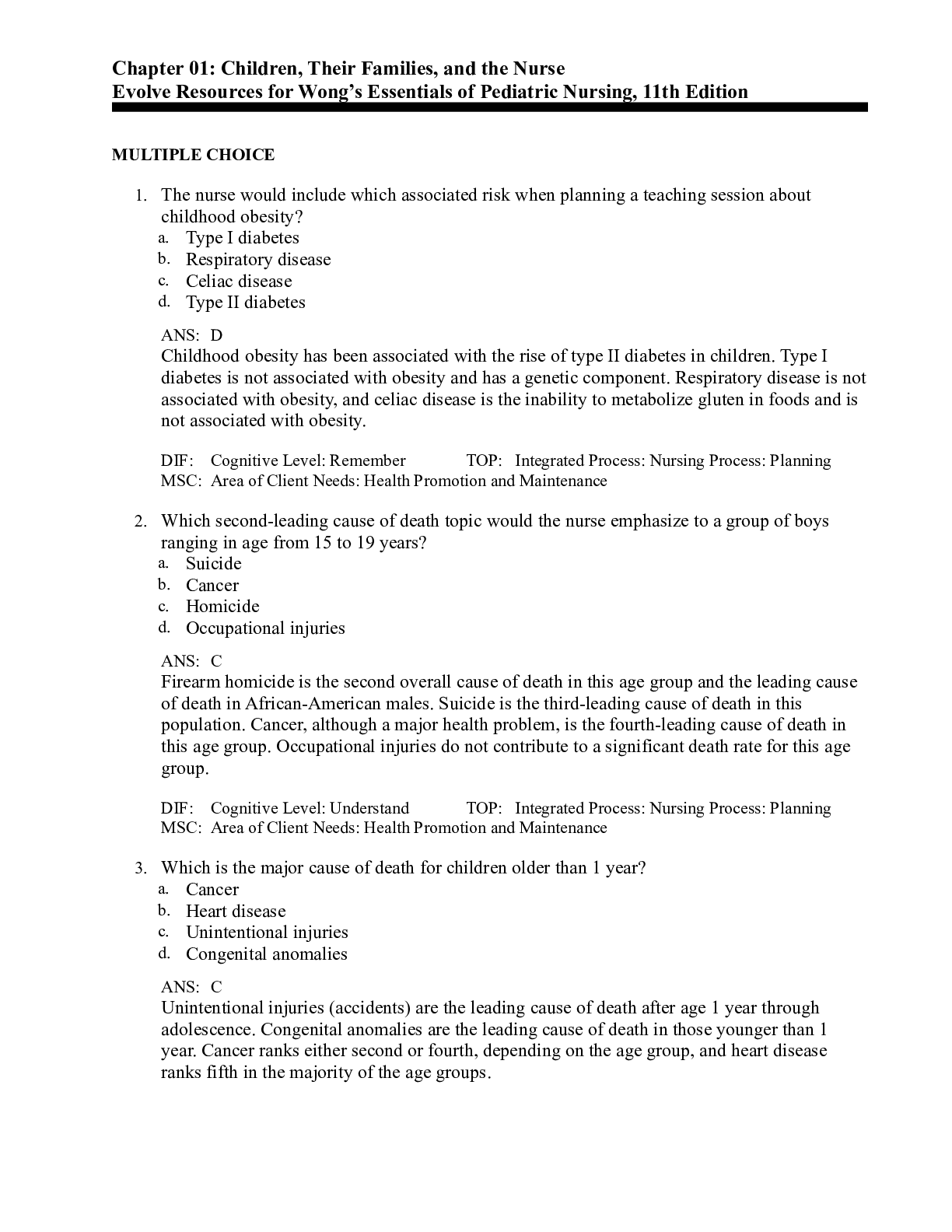
Wongs Essentials Of Pediatric Nursing 11th Edition Hockenberry...
$19
439 Pages
Textbook of Diagnostic Microbiology 6th Edition Connie; Donald...

$19
879 Pages
Understanding Medical Surgical Nursing 5th Edition Williams Al...


More related documents below