Airborne diseases - ANSWER Varicella, measles, TB
Contact diseases - ANSWER Impetigo, C-diff, MRSA, Scabies, Shigella
Droplet diseases - ANSWER Rubella, Influenza Type B, Mumps, Pneumonia, Pertussis, RSV
Standar
...
Airborne diseases - ANSWER Varicella, measles, TB
Contact diseases - ANSWER Impetigo, C-diff, MRSA, Scabies, Shigella
Droplet diseases - ANSWER Rubella, Influenza Type B, Mumps, Pneumonia, Pertussis, RSV
Standard Disease (No special precaution) - ANSWER HIV & Hepatitis B
ABG: If it's a respiratory problem it's a - ANSWER respiratory issues (respiratory ABG opposite PH 7.35-7.45 & HC03 22-26)
Normal HCO3 - ANSWER 22-26
Normal pH - ANSWER 7.35-7.45
Normal sodium levels - ANSWER 135-145
Normal potassium levels - ANSWER 3.5-5.0
Normal calcium levels - ANSWER 8.5-10.5
Normal creatinine levels - ANSWER 0.6-1.2
Normal INR range - ANSWER 2-3
Borborygmi - ANSWER Increased bowel sounds: a rumbling or gurgling noise made by the movement of fluid and gas in the intestines
If pH is low - ANSWER everything is low except potassium
- Bradycardia
- Decreased Bowel Sounds
- Hypotension
- Lethargy
- Flaccid
- Hyporefelxia (0 - 1+)
- Hyperkalemia
If pH is high - ANSWER everything is high except potassium
- Tachycardia/Tachypnea
- HTN (hypertension)
- Hyperreflexes (3+ 4+)
- Irritability
- Seizures (requires suctioning)
- Diarrhea
- Borborygmi
- Hypokalemia
In respiratory alkalosis - ANSWER pt is overventilating (Over 7.45)
In respiratory acidosis - ANSWER pt is underventilating (under 7.35)
ABG: When you don't know what to pick - ANSWER pick Metabolic Acidosis
Prolonged vomiting or suctioning cause - ANSWER Metabolic Alkalosis *everything else is acidosis
Ventilators: High pressure alarm - ANSWER Increased resistance check for
- Kinks in tubbing (unkink)
- Condensation in the dependent tubes (drain water)
- Mucus plugs (turn, cough, deep breath & then suction)
Ventilators: Low pressure alarm - ANSWER Decrease in resistance check for
- Main tube disconnect
- O2 sensor tube disconnect
In both cases reconnect the tube unless it is on the floor in this case bag pt and call respiratory
The number one psychological problem in ABUSE is - ANSWER Denial
Definition of denial - ANSWER Refusal to accept reality of their problem
Confront the pt with denial issues - ANSWER point out the difference between what they say and what they do... Example: You say you'r not an alcoholic but it's 10 am and you have already had a 6 pack of beer.
Don't say you - ANSWER say I (I seem to be frustrating you not you seem to be frustrated)
Grief and loss - ANSWER DABA (denial, arguing, bargaining and acceptance)
Manipulation - ANSWER the abuser gets the significant other to do things that can be harmful to the pt.
Treat manipulation by - ANSWER setting limits and enforcing them
Wernicke-Korsakoff syndrome - ANSWER - Psychosis induced by vitamin B1 or thiamine deficiency
- S&S include amnesia (memory loss) with confabulation (making up stories)
- DO NOT CONFRONT (Redirect the patient instead)
Characteristics of Wernicke-Korsakoff syndrome - ANSWER - It is preventable (Take B1)
- Arrestable: stop getting worse (take B1)
- Irreversible (70%)
Antabuse & Revia (disulfiram) - ANSWER Aversion therapy
- Reacts with alcohol to cause severe sickness
- Onset & duration 2 WEEKS
Antabuse & Revia (disulfiram) interactions - ANSWER Alcohol
Mouthwash
Aftershave
Colone & Perfumes
Bug Spray
Elixer Medications
Hand Sanitizer
Uncooked icings
(They can have the red wine vinegret)
Upper Drugs - ANSWER Caffeine
Cocain
PCP/LSD (Psychedelics/Hallucinogens
Methamphetamines
Adderall (ADD Drug)
S&S of upper drugs - ANSWER everything goes up
- tachycardia
- hypertension
- Euphoria
- restlessness
- irritability
- borborygmi
- +3 & +4 reflexes (hyper)
Downer drugs - ANSWER everything thats not an upper drug is a downer! (memorize the 5 uppers)
S&S of downer drugs - ANSWER - hypotension
- lethargy
- respiratory depression
- constipation
- bradicardia
After you know if the drug is an upper or a downer you assess for - ANSWER Overdose or withdrawal
- Overdose = too much
- withdrawal = not enough
If you have withdrawal of an upper medication - ANSWER you have too little
If you are withdrawing from a downer - ANSWER everything will be too high
- seizures
Overdose at birth - ANSWER always assume intoxication within the first 24hrs after 24hrs assume withdrawal
Alcohol withdrawal syndrome (AWS) - ANSWER 24hrs after stoping drinking
- not life threatening
- not a danger to self or others
- CARE: Regular diet, Simi privet any wear, up at liberty no restraints
Delirium Tremens (DT) - ANSWER 72hrs after stoping drinking
- life threatening
- A danger to self & others
- CARE: NPO or clear liquids, privet room near nurses station, fall risk, restraints
Treatment for Alcohol withdrawal syndrome - ANSWER Antihypertensive
Tranqulizer
Multi vitamin containing B1
Restraint used for Delirium Tremens (DT) patients - ANSWER Vest Restraint
Two point lock letters (Opposite hand and leg) Rotate 2 point restraints every 2 hrs
Aminoglycosides - ANSWER Antibiotics (when nothing else works) End in Mycin
NOT a Mycin - ANSWER Erythromycin
Erythromycin
Clarithromycin
If it has thro in it throw it off the aminoglycoside list
Top 5 drugs on NCLEX - ANSWER Psychiatric drugs
Insulin
Anticoagulants
Digitalis
Amino-glycosides
OTHERS
- Steroids
- BB
- CCB
- Pain Meds
- OB Meds
Toxic effects of aminoglycosides - ANSWER Ototoxic (Think Mice ears)
- Tinitus
- Hearing loss***
- Vertigo/dizziness
Nephrotoxicity (human ear looks like the kidney)
- monitor creatinine (24hr is better then the serum)
Toxic to cranial nerve number 8 and administer them every 8 hrs (Think Number 8)
Aminoglycoside Rout - ANSWER IM or IV (PO not absorbed only given for hepatic coma to reduce ammonia levels and pre op bowl surgery to sterilize the bowel)
Who can sterilize my bowels? - ANSWER Neo Can
- Neomycin
- Kanamycin
PO not absorbed only given for hepatic coma to reduce ammonia levels and pre op bowl surgery to sterilize the bowel
Peak Levels - ANSWER show the highest concentration drawn after administration
trough level - ANSWER lowest blood level of a drug drawn before next administration
When do you draw an IV med peak level - ANSWER 15-30min after bag is empty
When do you draw a SL (sublingual) peak level - ANSWER 5-10min after drug is dissolved
When do you draw an IM peak level - ANSWER 30-60 min after administration
Always draw trough - ANSWER 30 min before the next dose!!!
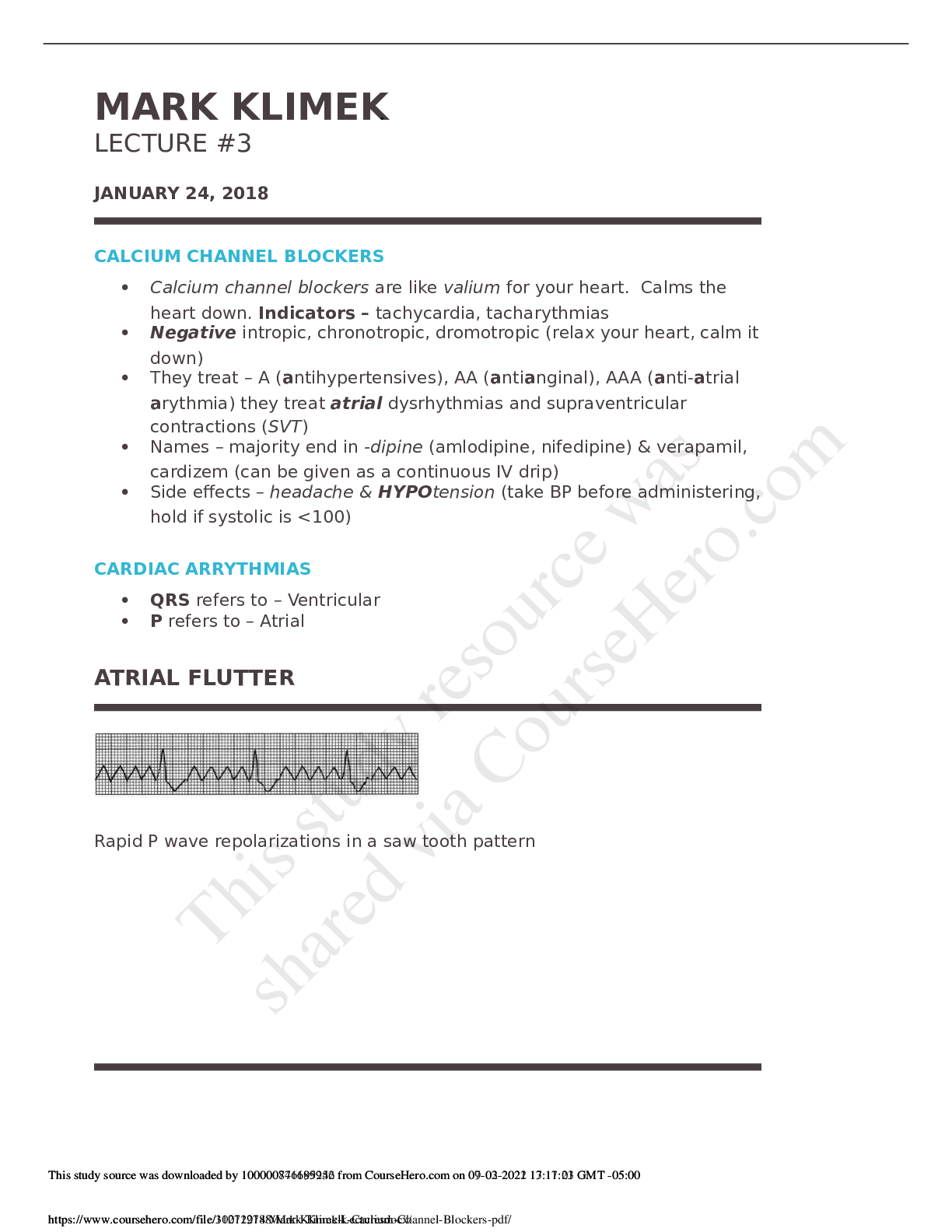
Calcium Channel Blockers - ANSWER Weaken, Slow down and depress the heart
Calcium channel blocker's treat - ANSWER A AA & AAA
- Anti Hypertensives
- Anti Angina (works by decreasing oxogen demand)
- Anti Atrial Arrhythmia (Atrial Flutter, Atrial Fibrillation and SVT is the only ventricular)
Calcium Chanel blocker adverse effects - ANSWER Headache
Hypertension
Always check on a select all that apply - ANSWER Headache!
names of calcium channel blockers - ANSWER Everything ending in -dipine
-verapamil
-cardazem (continuous IV drip)
What should you do before administering a calcium channel blocker - ANSWER Check BP
- hold medication if the systolic is under 100
Normal Sinus Rythym (NSR) - ANSWER P wave before every QRS and a T wave after every QRS complex and the QRS complexes are evenly spaced
ventricular fibrillation - ANSWER the rapid, irregular, and useless contractions of the ventricles (no pattern)
ventricular tachycardia - ANSWER a very rapid heartbeat that begins within the ventricles (pattern)
Asystole - ANSWER absence of contractions of the heart
QRS depolarization - ANSWER always ventricular
If it says P wave it's - ANSWER atrial unless it says lack of a P wave then its ventricular
No QRS - ANSWER asystole
Saw tooth - ANSWER flutter
Cyanotic = - ANSWER fibrillation
Bizarre - ANSWER tachycardia
Periodic wide, bizarre QRS's - ANSWER PVCs
PVC's - ANSWER Never reach high priority
PVC pt's are low priority unless there are more than 6 in a minuet, 6 in a row. then they are moderate priority.
lethal arrhythmias - ANSWER Asystole (No heart rate, flat line)
V fib
High priority!
potentially life-threatening arrhythmia - ANSWER V-tach
PVC and V tach treatment - ANSWER lidocaine and amiodarone
Atrial treatment - ANSWER ABCD's
- Adenocard
- Beta Blockers (olol)
- Calcium Channel Blockers
- Digitalis/Digoxin (lanoxin)
Lanoxin - ANSWER Digitalis/Digoxin
IV push - ANSWER When you don't know you go slow
IV push Adenocard - ANSWER Push FAST!!!!!
Beta Blockers - ANSWER -olol
(atenolol)
For Vfib you - ANSWER D fib (Shock them)
In a pneumothorax the chest tube removes - ANSWER air
In a hemothorax the chest tube - ANSWER removes blood
In a hemopneumothorax the chest tube removes - ANSWER air and blood
Chest tube location apical - ANSWER The chest tube is on top of the lung to remove air
Chest tube location basilar - ANSWER At the bottom of the lungs and remove blood
Unilateral - ANSWER one-sided
Bilateral - ANSWER both sides
Assume chest surgery is - ANSWER unilateral unless otherwise specified
pnumonectomy - ANSWER removal of a lung (NO CHEST TUBES NEEDED)
What do you give for Asystole - ANSWER Epi first then Atropine
What do you do if you knock over a Jackson-Pratt drain - ANSWER pick it up and have the pt take some deep breaths
What do you do FIRST if the seal of the chest tube breaks - ANSWER Clamp the tube
What do is BEST to do if the seal of the chest tube breaks - ANSWER Submerge tube in water
Person has Ventricle Fibrillation with no pulse what is the FIRST thing the nurse should do - ANSWER Place back board
Person has Ventricle Fibrillation with no pulse what is the BEST thing the nurse should do - ANSWER Start Chest Compressions
What do you do if the chest tube gets pulled out? - ANSWER 1. Cover it up with your gloved hand
2. Have someone prepare a sterile vasoline gauze
3. Do a switchout from holding the glove to putting the gauze over it
4. Put a dry sterile gauze over the vasoline gauze to tape it to the person
5. Tape it on 3 sides
What is the BEST thing to do when a chest tube gets pulled out? - ANSWER put a gasoline gauze over it
What is the FIRST thing to do when a chest tube gets pulled out? - ANSWER cover it with a gloved hand
Intermittent bubbling in the water seal chamber is - ANSWER GOOD
Continuous bubbling in the water seal chamber is - ANSWER BAD, an AIR LEAK (put tape over it to seal)
Intermittent bubbling in the suction control chamber - ANSWER BAD (suctioning is too low)
Continuous bubbling in the suction control chamber - ANSWER GOOD document bubbling
Congenital Heart Defect - ANSWER Trouble heart defect start with the letter T
- They will all have a murmur trouble or not
- Echocardiogram gram is done on all cardiac defects
TRouBLe heart defects blood shunt blood - ANSWER Right to Left (R before L in the word trouble)
What do you do if the seal of the chest tube breaks - ANSWER CLAMP IT
CUT the tube
SUBMERGE in water
UNCLAMP
(It's in alphabetical order)
Tetralogy or fallot symptoms - ANSWER VarieD PictureS Of-A RancH
- Ventricular Defect
- Pulmonary Stenosis
- Overriding Aorta
- Right Hypertrophy
Hep B transmission - ANSWER Hep Blood (blood transfusion)
Staph infection precautions - ANSWER Contact precaution
Hep A transmission - ANSWER Hep Anus (fecal oral)
Cushing's triad - ANSWER bradycardia, hypertension, and widening pulse pressure
Rule of 9's for burns - ANSWER 9 (head), (4.5/4.5)
18 (arms), (4.5 X4)
36 (thorax), (18X2)
36 (legs) (9 X 4)
1 (perineum) equal 99.
Warfarin (Coumadin) antidote - ANSWER Vitamin K
Heparin antidote - ANSWER protamine sulfate
How do you measure crutches - ANSWER 2-3 finger widths below the anterior axillary fold to a point lateral to and slightly in front of the foot
elbow flexion on properly fitted crutches - ANSWER 30*
Two point gate - ANSWER move a crutch and an opposite foot together
Three point gate - ANSWER move two crutches and the bad leg together
Four point gate - ANSWER move everything separately (very slow but very stable)
Swing through gait - ANSWER for non weight barring (move both crutches at the same time as a bad leg)
Use 4 point gate for a - ANSWER sever problem (sever bilateral weaknesses)
Use a 2 point gate for - ANSWER miles problems (mild bilateral weaknesses)
When to use a crutch gate - ANSWER odd for odd and even for even
- 1 leg is effected use an odd point gate (1 & 3)
- 2 legs are effected use a even point gate (2 & 4)
Crutches - ANSWER up with the good down with the bad
- when you go down the stairs start with the bad
- when you go up the stairs start with the good
Cane ambulation - ANSWER hold the cane on the STRONG side
Walkers and bags - ANSWER tie stuff to the side NOT the front
- Do not put wheels on walkers
Nerotic = - ANSWER non psychotic
Contact precaution - ANSWER - Privet room preferred unless pt has the same disease
-
Walkers - ANSWER pick them up set them down walk to them
psych patients - ANSWER are they psychotic or non psychotic
Delusion - ANSWER False fixed idea or belief
Hallucination - ANSWER False, fixed sensory experience.
- auditory (sound) Example: I hear demon voices
- visual (sight)
- tactile (feeling)
- gustatory (taste)
- olfactory (smelling)
Illusions - ANSWER False, fixed sensory experience with a referent
- There is actually something there but they miss intemperate it... Example: The client hears the nurses talking and says "I hear demon voices"
Functional Psychosis - ANSWER schizophrenia, schizo affective, major depression, mania
pt has potential to learn reality
Psychotic Patients - ANSWER Dementia, Seniel, Delirium
- Redirect them
- Re orientate to person, place and time but not to reality about the situation they are confused about
Functional Psychotic - ANSWER Potential to learn reality
- Acknowledge feeling
- Present reality
- Set a limits (Stop talking about...)
- Enforce limits
delirium tremens - ANSWER a disorder involving sudden and severe mental changes or seizures caused by abruptly stopping the use of alcohol (Therapeutic response: You Are Safe)
[Show More]